Carpal tunnel syndrome isn’t just a tingling hand-it’s a sign your median nerve is being squeezed. Every year, over half a million Americans undergo surgery for it. But most don’t need to. The truth? Early action can stop it before it ruins your grip, your sleep, or your job. If you’ve been waking up with numb fingers or struggling to button your shirt, this isn’t something you should ignore.
What Exactly Is Carpal Tunnel Syndrome?
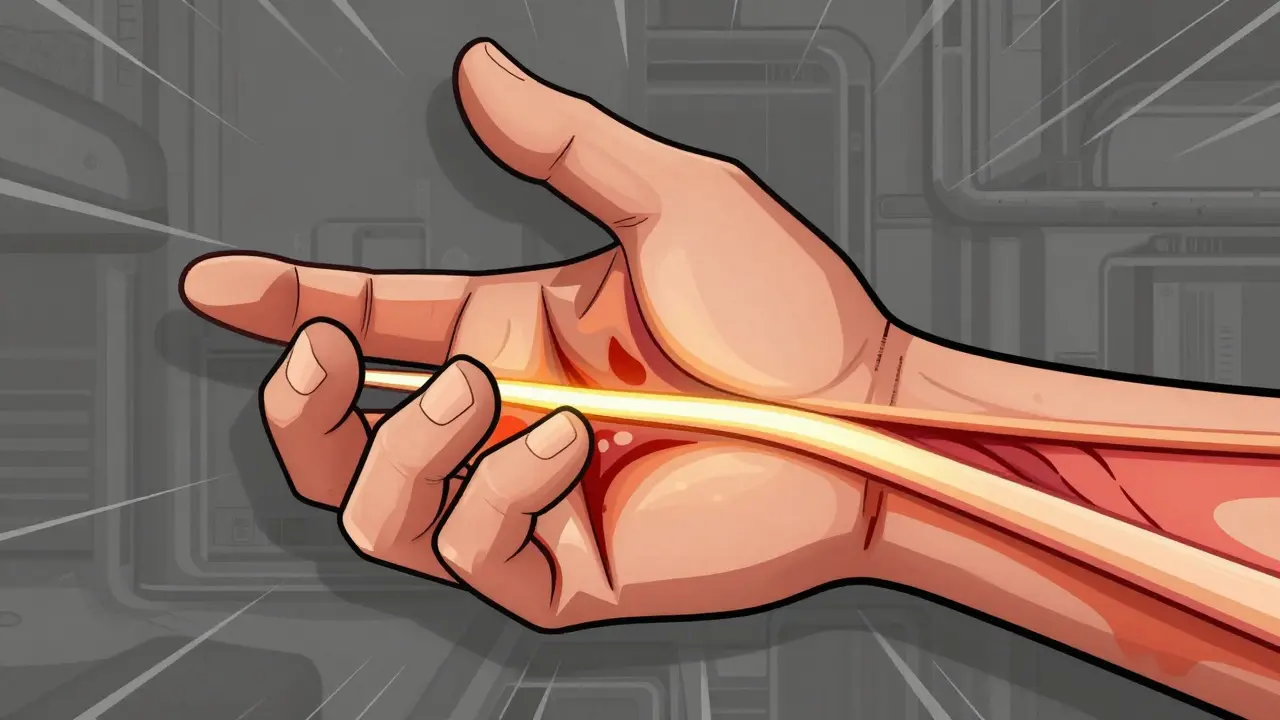
Carpal tunnel syndrome happens when the median nerve gets compressed as it passes through a narrow passage in your wrist called the carpal tunnel. This tunnel isn’t empty-it holds nine tendons that bend your fingers and thumb, plus the median nerve. When swelling happens inside this tight space, the nerve gets pinched. That’s when numbness, tingling, and pain start.
The symptoms follow a clear pattern. At first, you might feel it only at night-your hand wakes you up. Shaking it helps. Then, daytime activities become harder. Holding a coffee cup, typing, or driving starts to feel awkward. In advanced cases, your thumb muscles weaken. You drop things. You can’t tell if you’re holding a pen or a coin. That’s not just discomfort-it’s nerve damage.
Women between 45 and 60 are three times more likely to get it than men. People in jobs that involve repetitive hand motions-like assembly line workers, healthcare staff, or cashiers-are at higher risk. But it’s not just about work. Pregnancy, diabetes, thyroid issues, and even genetics can play a role.
How Do You Know It’s Carpal Tunnel and Not Something Else?
Not every hand numbness is carpal tunnel. Arthritis, neck problems, or even a pinched nerve in your elbow can mimic the symptoms. That’s why diagnosis needs more than just a guess.
Doctors use a mix of physical tests and objective measures. The Phalen test-where you hold your wrists bent for a minute-can trigger tingling if the nerve is compressed. The Tinel sign-tapping over the wrist-might make your fingers shock. The carpal compression test, pressing directly on the tunnel, is even more reliable.
They’ll also ask you to mark your symptoms on the Katz hand diagram. If the numbness covers your thumb, index, middle, and half your ring finger, it’s classic carpal tunnel. The other half of the ring finger? That’s the ulnar nerve-different problem.
For unclear cases, nerve conduction studies are the gold standard. If the median nerve takes longer than 3.7 milliseconds to send a signal across the wrist, that’s diagnostic. But here’s the catch: 15-20% of people over 60 have abnormal test results but no symptoms. That’s why doctors don’t rely on tests alone. They match the test to your real-life symptoms.
Stage 1: Mild Symptoms-Start Here
If you’re in the early stage-nighttime numbness, no muscle weakness-your best move is conservative treatment. And the #1 recommendation? A wrist splint worn at night.
Studies show 60-70% of people with mild to moderate carpal tunnel see big improvement after wearing a splint for just 4-6 weeks. The key? Keeping your wrist straight. Not bent forward, not bent back. Neutral. That takes pressure off the nerve while you sleep. Custom splints cost $150-$250, but basic ones from the drugstore work too if they hold your wrist properly.
Pair the splint with nerve gliding exercises. These aren’t stretches for your muscles-they’re gentle movements that help the nerve slide through the tunnel. A physical therapist can show you how in 2-4 sessions. Do them daily. They’re cheap, safe, and backed by solid evidence.
Also, change your habits. Avoid bending your wrist past 30 degrees for long periods. If you type, raise your keyboard so your wrists stay flat. If you hold a phone, switch hands. Even small adjustments matter.
Stage 2: Moderate Symptoms-Add Injections
If splinting and exercises aren’t enough after 6-8 weeks, the next step is a corticosteroid injection. This isn’t a cure, but it’s a reset button.
Injected directly into the carpal tunnel, the steroid reduces swelling around the nerve. About 70% of patients get relief that lasts 3-6 months. It’s not permanent, but it can buy you time. For people with symptoms under 10 months, conservative treatments like this work 75% of the time. After 12 months? That drops to 35%.
Some people get one injection. Others need two, spaced weeks apart. Side effects are rare but can include temporary pain at the injection site or a spike in blood sugar if you’re diabetic. It’s not for everyone-but if you’re trying to avoid surgery, it’s a smart option.
Stage 3: Severe Symptoms-Surgery Is the Answer
If you’ve lost feeling in your fingers, your thumb muscles are shrinking, or you can’t hold a glass without dropping it, you’re in the danger zone. Nerve damage at this stage can become permanent. That’s when surgery becomes necessary.
There are two main types: open release and endoscopic release. Open release means a 2-inch cut along the palm. Endoscopic uses one or two tiny cuts and a camera to cut the ligament from inside. Both have the same success rate: 90-95% of patients get lasting relief.
Endoscopic surgery might cost 15-20% more, but recovery is faster. Most people return to light work in 2-3 weeks instead of 4-6. Open release has a slightly higher chance of scar tenderness, but both can cause pillar pain-tenderness on the sides of the palm. That affects 15-30% of patients and usually fades in 6-12 weeks.
Complications like nerve injury are rare-under 1%. But don’t rush into surgery. If you’ve only had symptoms for a few months, try everything else first. If you’ve had them for over a year, don’t wait. The longer you delay, the less likely you are to get your hand back.
What About Newer Treatments?
There’s a new option called ultrasound-guided percutaneous release. The FDA approved it in 2021. A tiny knife, guided by real-time ultrasound, cuts the ligament through a needle-sized opening. No big cut. No stitches. Patients report 40% less pain and return to work 50% faster than with traditional surgery.
Ultrasound itself is also becoming a diagnostic tool. Measuring the median nerve’s size at the wrist-anything over 12mm²-is 92% accurate at spotting carpal tunnel. That means fewer nerve tests and quicker answers.
But these aren’t magic bullets. They’re tools for specific cases. Most people still do best with the tried-and-true: splints, exercises, injections, and surgery when needed.
Costs and Recovery: What to Expect
Conservative care-splint, therapy, one injection-usually costs $450-$750 out-of-pocket. Surgery? With insurance, expect $1,200-$2,500. Endoscopic runs a bit more. Without insurance, it can hit $8,000-$10,000.
Recovery isn’t instant. After surgery, you’ll need 6-8 physical therapy sessions over 4-6 weeks. Light-duty work? Two to three weeks. Full-duty work? Six to eight weeks. If you’re a construction worker or chef? Plan for 10-12 weeks.
And yes, it’s worth it. On RealSelf, 89% of people who had surgery say it was “worth it.” The ones who regret it? Usually those who waited too long.
Prevention Is Possible
You can’t always stop carpal tunnel-but you can reduce your risk. If your job demands repetitive motion, take breaks every 20 minutes. Stretch your wrists. Use ergonomic tools. Keep your wrists neutral. Don’t rest them on hard edges while typing.
And if you’re pregnant or have diabetes, monitor your symptoms closely. Hormonal changes and high blood sugar increase swelling. Catch it early, and you might avoid surgery entirely.
CTS isn’t a death sentence. It’s a signal. Listen to it before your hand forgets how to work.
Can carpal tunnel syndrome go away on its own?
Sometimes, yes-but only in very mild cases. If symptoms are brief, like occasional nighttime tingling during pregnancy, they often resolve after delivery. But if symptoms last more than a few weeks or start affecting your daytime activities, they won’t disappear without treatment. Waiting too long increases the risk of permanent nerve damage.
Is carpal tunnel syndrome caused by typing too much?
Not directly. While repetitive hand motions can contribute, studies show typing alone isn’t the main cause. More common triggers include forceful gripping, prolonged wrist flexion, vibration, and jobs that require constant hand use-like assembly line work, hairdressing, or healthcare. People who type all day but keep their wrists neutral rarely develop it.
Do wrist braces really help carpal tunnel?
Yes-especially at night. Wrist braces keep your wrist in a neutral position, reducing pressure on the median nerve. Clinical guidelines show 60-70% of people with mild to moderate carpal tunnel improve significantly after 4-6 weeks of consistent use. The key is wearing it every night, not just when it hurts.
How long does carpal tunnel surgery recovery take?
Most people return to light tasks in 2-3 weeks. Full recovery, including grip strength and no pain, takes 6-8 weeks. Endoscopic surgery may shorten this by 2-3 weeks compared to open release. Manual laborers may need 10-12 weeks before returning to heavy work. Physical therapy helps speed up the process.
Can carpal tunnel come back after surgery?
It’s rare-less than 5% of patients experience recurrence. Most cases of recurring symptoms are due to incomplete release during surgery or new injuries. If symptoms return after surgery, it’s usually not the original carpal tunnel coming back, but something else like scar tissue or a new nerve issue. A follow-up exam is needed to find out why.
Are there any natural remedies for carpal tunnel?
Nothing has been proven to cure it. Stretching, yoga, and acupuncture might help with mild discomfort, but they don’t reduce nerve compression. Supplements like B6 or turmeric have no strong evidence behind them. The only proven natural approach is modifying how you use your hands-avoiding positions that bend the wrist, taking breaks, and using ergonomic tools.
When should I see a doctor about carpal tunnel?
See a doctor if symptoms last more than two weeks, wake you up at night, or start interfering with daily tasks like buttoning clothes or holding objects. If you notice thumb weakness or muscle loss at the base of your thumb, don’t wait-this is a sign of advanced nerve damage. Early treatment prevents permanent problems.












i’ve had this for years and just ignored it till i dropped my coffee mug one morning-turns out, my thumb was half-dead. splint for 6 weeks, no surgery. life changed.
January 16Chelsea Harton